Dyslexia in children: understand, support, and help through singing
LANGUAGE DISORDERS
Your child mixes up b and d, reads twice as slowly as their peers, comes home exhausted every evening. Singing does not cure dyslexia. But used wisely, alongside a proper speech-language assessment, it activates several of the brain circuits the act of reading relies on.
Your child is in 2nd grade. They tell you they hate reading. They read "pordre" instead of "porte", skip the next word, start the line over. By evening, they shut the book the moment they can. Their teacher has hinted: "You might want to have them assessed." At midnight, stomach in knots, you type "child dyslexia" and land on ten lookalike sites.
CALYP and Adeline Toniutti have been supporting dyslexic children for over ten years. Singing, properly framed, comes as a complement to speech-language therapy: it activates several of the brain circuits the reading act relies on (phonological awareness, articulation, phonological memory, rhythm), inside an artistic setting where the child rebuilds confidence and the pleasure of learning.
DEFINITION
What exactly is dyslexia?
Dyslexia is a specific learning disorder of reading. The DSM-5 classifies it among "Specific Learning Disorders" (315.00; ICD-11: 6A03.0). "Specific" means: the disorder cannot be explained by intellectual deficit, sensory impairment, lack of teaching, or unfavorable environment. A dyslexic child can be highly intelligent, deeply curious, and well stimulated. The reading machine, in their case, simply works differently.
In practical terms, the child takes much longer to associate a letter with the sound it represents. Where an expert reader decodes automatically, the dyslexic child must make an effort on every word. They tire. They guess. They invent. They avoid. Reading, which should become transparent by 2nd grade, remains a feat of strength.
Prevalence is estimated at 6 to 8% of school-age children, roughly one child per classroom. It is neither rare nor a passing trend: we simply talk about it more since the 2000s. (Source: Inserm, French National Institute for Health and Medical Research.)
Three misconceptions to clear up right away
- Dyslexia is not an intellectual delay. No correlation with IQ.
- Dyslexia is not a lack of motivation. A child who "is not trying" is, nine times out of ten, a child trying three times harder than the others for a visibly poorer result.
- Dyslexia is not caused by screens, nor by failed parenting. The factors are neurological and genetic. More on that below.
SIGNS TO WATCH FOR
The warning signs by age
No single sign on its own indicates dyslexia. But their accumulation, especially after one term of 1st grade (CP), justifies an assessment.
Age 5, kindergarten
Before reading begins
- The child does not play with rhymes ("cat / bat / hat" leave them cold).
- They struggle to break a word into syllables by clapping.
- They cannot identify the initial sound of a word ("what sound do you hear at the start of boat?").
- They mix up the order of words in simple sentences.
Age 6–7, 1st grade / start of 2nd grade (CP / CE1)
When it becomes visible
- Confusion of visually similar letters: b / d / p / q, m / n.
- Confusion of similar sounds: t / d, k / g, f / v.
- Syllable inversions: "pordre" for "porte", "al" for "la".
- Very slow reading, syllable by syllable, even on familiar words.
- The child guesses the end of a word after decoding the beginning.
- Refusal to read aloud, sometimes tears before homework.
Age 8–10, 3rd to 5th grade (CE2 / CM)
When the gap settles in
- Reading still labored, twice as slow as the rest of the class.
- Disastrous spelling, even on words seen a thousand times.
- Understands instructions better when read aloud than when reading them alone.
- Intense fatigue at the end of a school day.
- First avoidance signs: morning stomachaches, refusal to go to school.
- Self-esteem collapses: "I'm hopeless".
Middle school, high school
What teenagers experience
- Systematic avoidance of anything to be read (novels, manuals, exam prompts).
- Very strong orally, in free fall in writing.
- Difficulty with foreign languages (English in particular).
- Performance anxiety, sometimes mild depression around age 14–15.
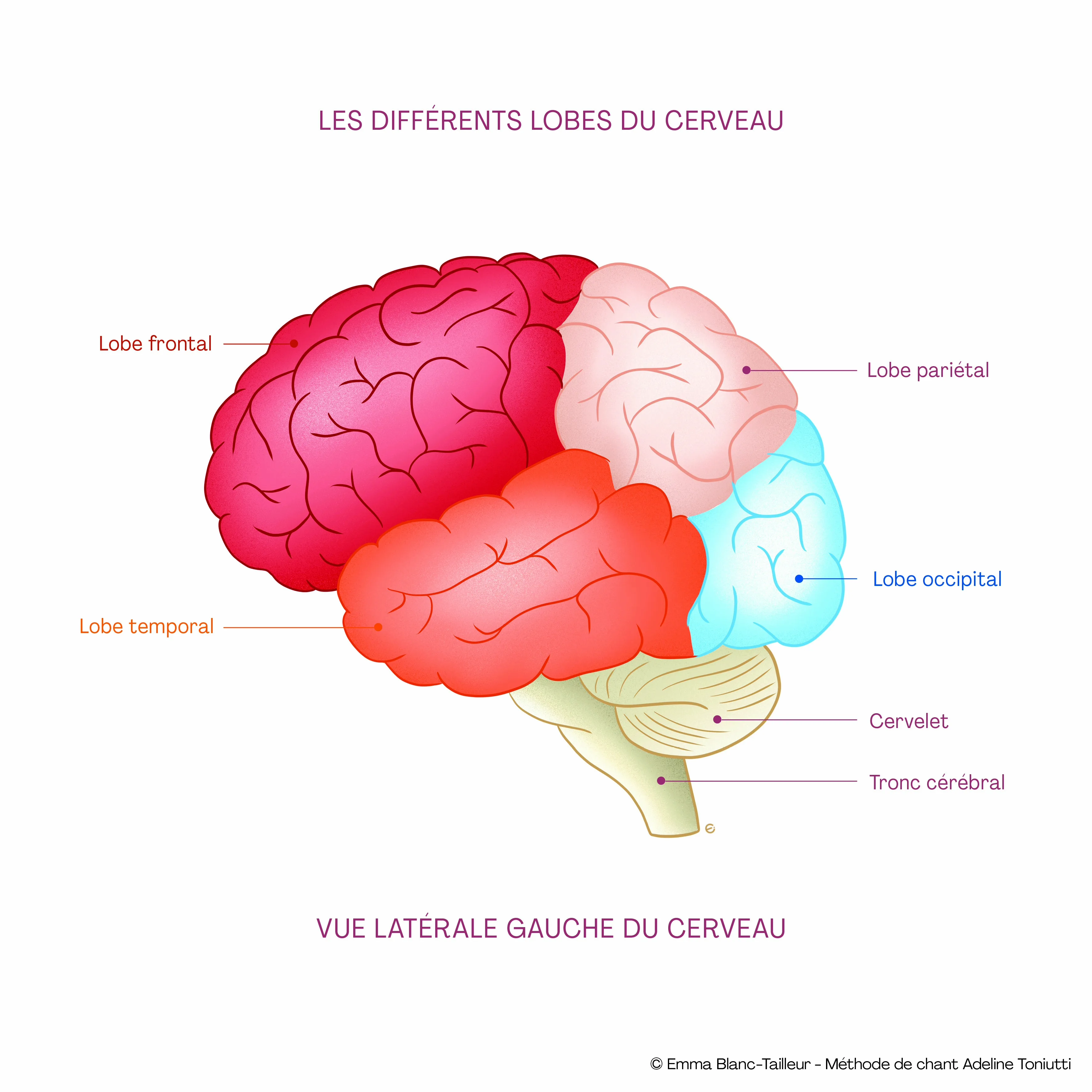
© Emma Blanc-Tailleur, illustration of Adeline Toniutti's method, Anatomy of Singing
CAUSES
Where does dyslexia come from?
Dyslexia is, above all, neurological. Imaging studies show a different functioning of the left occipito-temporal area, what researchers call the "letterbox of the brain" (Stanislas Dehaene), as well as different connectivity with Broca's area (language production) and Wernicke's area (comprehension).
It is also strongly genetic. If one parent is dyslexic, the child has a 40 to 60% risk of being dyslexic too. Several genes have been identified (DCDC2, KIAA0319, ROBO1).
It is not caused by parenting, screens, a school change, or a divorce. Context can worsen a dyslexia that already existed; it does not create it.
SCIENTIFIC INSIGHT
We are born with a fixed capital of neurons. The connections between them, however, adapt throughout life depending on stimulation and lifestyle. The brain is not made of frozen zones but of interconnected networks, with a mapping almost unique to each person, a bit like a fingerprint.
When we hear music, the memory and emotion areas activate from the very first second, whether we are aware of it or not. When we sing, the fine motor activity of the face, tongue and vocal cords joins in, and that whole circuit talks to the language areas.
DIAGNOSIS
Who to see, at what age, and in what order?
According to the recommendations of the French National Authority for Health (HAS), a diagnosis is rarely made before the end of 1st grade (CP), and more typically in 2nd grade (CE1). Before then, we speak of a delay or learning difficulty: the brain needs time to settle into reading. If at seven or eight, despite conventional teaching, reading remains laborious, the assessment is launched.
The usual order:
- The general practitioner or pediatrician. First point of entry. They guide the family and write the first prescriptions.
- An ENT and audiometric assessment. Crucial, and too often overlooked. A child who hears poorly, chronic glue ear, mild deafness, shows exactly the same signs as a dyslexic child. Before going further, this lead must be ruled out.
- A full speech-language assessment. The central exam. The speech-language pathologist (SLP) evaluates reading, spelling, phonological awareness, working memory, rapid naming. The assessment lasts between 1.5 hours and three sessions.
- If needed, a neuropsychological assessment. To confirm there is no other associated disorder (ADHD, dyscalculia, gifted profile, anxiety). About 40% of dyslexic children have an associated disorder.
At the end of the assessment, the SLP either confirms or rules out the diagnosis. If dyslexia is confirmed, therapy is set up, generally one to two sessions per week, over one to three years, sometimes longer depending on severity.
THE CALYP APPROACH
Why singing helps dyslexic children
Singing is a powerful trigger for progress, both for brain activity and for bodily and emotional engagement. At CALYP, it is a complement to speech-language therapy: it stimulates several of the brain areas involved in reading, inside an artistic, positive and caring setting where the child rebuilds confidence.
1. Phonemic awareness, through the ear
Dyslexia is, above all, a phonological disorder: the child struggles to manipulate the basic sounds of the language. When you sing "Ba-ta-clan" or "um-brel-la" on a beat, the brain breaks down the syllable without conscious effort, because the melody forces it to. Singing trains phonemic awareness through play, where speech therapy trains it through exercise.
2. Rhythm: the missing backbone
Adeline's method gives dyslexic children a precise technique, tested over ten years and set out in Anatomy of Singing: mentally spatialize the musical phrase from right to left, alternating, one beat right, one beat left. This alternation creates rhythmic stability. The tempo is marked with parallel hands: low hand for the strong beat, high hand for the offbeat. The child rediscovers a regularity that, in their reading, has never existed.
3. Articulation, in the flesh
The CALYP method works consonants by family, the way an osteopath works joints: B / P at the lips, D / L / T at the tip of the tongue behind the upper teeth, F / S / SH on exhaled air. The child puts a hand to their mouth, feels the vibration, watches in the mirror the tongue touching or not touching. The articulatory gesture becomes visible, palpable. For a child confusing t and d, it is a revelation.
4. Working memory, stretched by the song
Learning the lyrics of a song trains short-term phonological memory, precisely the channel most deficient in dyslexics. Three verses and a chorus is thirty to forty phrases the brain holds in a loop. The song sticks. Reciting does not. Many parents tell us their child remembers "Twinkle Twinkle Little Star" perfectly but stumbles on the four times table, that is exactly this phenomenon.
5. Self-esteem, never overlooked
By age 8, a dyslexic child has already been told a hundred times that they "don't listen", "don't try", are "lazy". When they arrive at a session with Adeline or a CALYP-trained coach, they are not asked to read. They are asked to sing. And there, they discover they are good at something visible, audible, recordable to show grandma. The school benefit goes through that door first. Neuroscience confirms it: an anxious brain learns badly. A brain that feels competent learns.
AT SCHOOL
School accommodations: PAP, PPS, MDPH (and the US/UK equivalents)
In France, two main systems exist. (In the US, the closest equivalents are the IEP, Individualized Education Program, and the 504 plan; in the UK, the Education, Health and Care Plan or SEN Support.)
- The PAP (Personalized Support Plan). Internal to the school, no need to go through the MDPH. Decided between the parents, the school doctor and the head teacher. It allows: extra time, enlarged photocopies, instructions read aloud, computer use, exemption from reading aloud. Suited to mild and moderate dyslexias. (Closest US equivalent: the 504 plan.)
- The PPS (Personalized Schooling Project). Heavier process, goes through the MDPH (Departmental Center for Disabled Persons). Recognizes a disability, opens the right to an AESH (school support assistant), to adapted equipment, and to accommodations during national exams (brevet, baccalaureate). Suited to severe dyslexias or associated disorders. (Closest US equivalent: the IEP.)
In middle and high school, these accommodations continue and notably allow extra time on national exams. Many dyslexic students graduate without difficulty thanks to these supports, they just need to ask for them.
FREQUENTLY ASKED QUESTIONS
What parents ask us most
At what age can dyslexia be diagnosed?
Officially, from about six months into 1st grade, around March-April of the 1st-grade year, so age 6 and a half. Before that, we speak of a delay or learning difficulty. That said, as early as the final year of kindergarten, certain signs (poor phonological awareness, difficulty syllable-segmenting) can prompt heightened vigilance and justify monitoring.
Can dyslexia be cured?
No. Dyslexia is a neurological way of functioning that lasts a lifetime. However, with early speech-language therapy, school accommodations and compensation strategies (singing among them), a dyslexic child can absolutely pursue long studies and become a lawyer, doctor, or researcher. Many brilliant adults are dyslexic and barely notice it day to day.
My child swaps b and d, is that necessarily dyslexia?
Not necessarily. The b/d confusion is normal at the start of 1st grade, until late 1st grade (April-May). If it persists massively after the start of 2nd grade, it is a sign to take seriously. But on its own, it does not establish dyslexia. The speech-language assessment remains the reference exam.
Can singing replace speech-language therapy?
No, never. Speech-language therapy is the reference treatment and must be maintained as long as the speech therapist recommends. Singing is a complement, to work on phonemic awareness through play, on rhythm, articulation and, perhaps above all, self-esteem. At CALYP we always work with the speech therapist, never instead.
My child is 6 and sings out of tune, is that a sign?
Not at all. Singing in tune is something one learns; it is not a gift. Many dyslexic children sing very well, music is often a domain where they shine, because it does not depend on reading. And those who sing out of tune at 6 can perfectly well sing in tune at 9 with a little coaching.
Is dyslexia hereditary?
Yes, strongly. If one parent is dyslexic, the child has a 40 to 60% risk of being dyslexic too. Twin studies confirm heritability around 50–70%. Several genes have been identified (DCDC2, KIAA0319, ROBO1). This explains why several siblings can be affected within the same family.
Is there a reliable online test?
No. No online test replaces a speech-language assessment. Early-screening tools for spoken language exist in preschool (used by school doctors and pediatric services), they do not diagnose dyslexia itself but can flag language fragility. Be wary of websites that claim to "diagnose" your child online.
My child does not enjoy singing, can it still work?
Often, the child who "does not enjoy singing" is mostly afraid of singing badly in front of someone. The individual session, in a kind setting, lifts that fear within a few sessions. If the child still stays closed off after five or six sessions, we do not push, other approaches exist (drama, music therapy). What matters is that they have at least one place in their week where they feel good at something.
Should I tell the teacher?
Yes, as soon as possible. A teacher who knows is an ally. A teacher in the dark can, without meaning to, worsen the child's distress by thinking them lazy or distracted. Ask for a meeting with the class teacher right after the diagnosis, and provide the speech therapy report along with the accommodation request.
How do I know if my child has an associated disorder (ADHD, dyspraxia)?
About 40% of dyslexic children have another associated disorder: ADHD (attention deficit), dyspraxia (coordination disorder), dyscalculia (math disorder), mild autism spectrum profile. If the speech therapist or the teacher suspects it, a full neuropsychological assessment will map out strengths and weaknesses precisely. This assessment lasts about 4 to 6 hours and is generally not reimbursed.
SOURCES & REFERENCES
This page is built on medical and peer-reviewed sources
All factual claims on this page (diagnostic codes, prevalence, genetics, neuroanatomy of reading, comorbidities, recommendations, school systems) come from verified scientific sources: institutional recommendations (HAS, Inserm, APA, WHO), indexed peer-reviewed articles (PubMed, Nature, Brain, PLOS) and official classifications (DSM-5 APA, ICD-11 WHO).
Official classifications and diagnostic definitions
- American Psychiatric Association (APA), Specific Learning Disorder, DSM-5 fact sheet. View the APA factsheet
- World Health Organization (WHO), ICD-11, 6A03 Developmental learning disorder, in force since January 1, 2022. View the WHO page
Official recommendations and collective expert reviews
- Haute Autorité de Santé (HAS, French National Authority for Health), How to improve the care pathway for a child with specific language and learning disorders, guide validated December 2017. Read the PDF guide
- Inserm (French National Institute for Health and Medical Research), Dyslexia, dysorthographia, dyscalculia: review of scientific data. Collective expert report, Inserm editions, 2007. Consult on iPubli-Inserm
- Inserm, Scientific dossier Specific learning disorders. View the dossier
Peer-reviewed articles, neurobiology and brain imaging
- Dehaene S, Cohen L, The unique role of the visual word form area in reading, Trends in Cognitive Sciences, 2011, 15(6):254-262. View on PubMed
- Ramus F, Developmental dyslexia: specific phonological deficit or general sensorimotor dysfunction?, Current Opinion in Neurobiology, 2003, 13(2):212-218. View on PubMed
- Ramus F, Rosen S, Dakin SC, Day BL, et al., Theories of developmental dyslexia: insights from a multiple case study of dyslexic adults, Brain, 2003, 126(Pt 4):841-865. View on PubMed
Peer-reviewed articles, genetics of dyslexia
- Schumacher J, Hoffmann P, Schmäl C, Schulte-Körne G, Nöthen MM, Genetics of dyslexia: the evolving landscape, Journal of Medical Genetics, 2007, 44(5):289-297. Read on PubMed Central
- Carrion-Castillo A, Franke B, Fisher SE, Molecular genetics of dyslexia: an overview, Dyslexia, 2013, 19(4):214-240. View on PubMed
- Snowling MJ, Melby-Lervåg M, Oral language deficits in familial dyslexia: a meta-analysis and review, Psychological Bulletin, 2016, 142(5):498-545. View on PubMed
- Doust C, Fontanillas P, Eising E et al., Discovery of 42 genome-wide significant loci associated with dyslexia, Nature Genetics, 2022, 54(11):1621-1629. View on Nature Genetics
Peer-reviewed articles, comorbidities (ADHD, anxiety, self-esteem)
- Germanò E, Gagliano A, Curatolo P, Comorbidity of ADHD and dyslexia, Developmental Neuropsychology, 2010, 35(5):475-493. View on PubMed
- Mugnaini D, Lassi S, La Malfa G, Albertini G, Internalizing correlates of dyslexia, World Journal of Pediatrics, 2009, 5(4):255-264. View on Springer
Peer-reviewed articles, music, rhythm and reading
- Flaugnacco E, Lopez L, Terribili C, Montico M, Zoia S, Schön D, Music Training Increases Phonological Awareness and Reading Skills in Developmental Dyslexia: A Randomized Control Trial, PLOS ONE, 2015, 10(9):e0138715. Read on PubMed Central
- Patel AD, Why would Musical Training Benefit the Neural Encoding of Speech? The OPERA Hypothesis, Frontiers in Psychology, 2011, 2:142. Read on PubMed Central
This page is for information purposes. It does not replace individual medical advice. If in doubt about your child's language development or learning, please consult a doctor (general practitioner, pediatrician or school doctor) and a speech-language pathologist.
GOING FURTHER
Explore the topic in more depth
PARENT PAGE
Language disorders
Overview: language delay, dyslexia, dysphasia, ADHD, dyspraxia. The CALYP method and neuroscience.
CLINIC
Voice Clinic
CALYP's voice clinic: medical specialists, vocal rehabilitation, and the CALYP method backed by 26 doctors.
ABOUT
Adeline Toniutti
Founder of CALYP, vocal coach, author of Anatomy of Singing, ten years of experience with dyslexic children.
GET IN TOUCH
Contact us
Book a discovery session in person in Paris or remotely. Reply within 24 hours.
IF YOU HAVE A DOUBT
Book a first lesson
At CALYP, sessions are playful, designed to rebuild children's confidence inside an artistic, positive and caring setting, and to spark new progress thanks to what the musical gesture awakens. A complement to speech-language therapy, never a substitute. First discovery session with Adeline or a CALYP-trained coach, in person in Paris or remotely.
Book a first lesson