Dyslexia or dysphasia: how to tell them apart?
CHILD LANGUAGE DISORDERS
Two disorders often confused, two very different logics. Dyslexia affects reading; dysphasia (Developmental Language Disorder, DLD) affects oral language. Comparison table, ages of onset, and who to consult.
Dyslexia and dysphasia: two words that look alike, and for good reason. They share the same Greek prefix dys-, which signals a dysfunction or difficulty. But they do not refer to the same thing: dyslexia affects reading; dysphasia, known internationally today as Developmental Language Disorder (DLD), affects oral language. Different age of onset, different care pathway.
The difference fits in one line: dyslexia is a reading disorder that emerges around age 6-7 when formal reading begins. Dysphasia (DLD) is an oral-language disorder visible from early childhood. The rest of this page unpacks that line, with a comparison table, two clinical definitions, and a clear path forward depending on what you observe in your child.
DIRECT COMPARISON
Dyslexia vs dysphasia (DLD): 9 points to tell them apart
A single table to put each disorder in its place. Read it row by row before going further.
| Criterion | Dyslexia | Dysphasia (DLD) |
|---|---|---|
| Definition | A specific, persistent disorder of reading and written transcription. | A structural, persistent disorder of oral language, production, comprehension, or both. |
| What is affected | Decoding written sounds: frequent confusion of visually similar letters (b/d, p/q), especially early on, syllable inversion, very slow reading, unstable spelling (dysorthographia). | The very building of sentences: poor vocabulary, telegraphic syntax (“me no want”), distorted words, sometimes impaired comprehension. |
| Age of onset | Visible at the start of formal reading instruction, around age 6-7. Diagnosis is made after at least 18 months of instruction, generally around age 7-8. | Visible from 18-30 months, sometimes earlier. Firm diagnosis usually made between ages 4 and 6 after repeated assessments. |
| Who makes the diagnosis | Speech-language pathology assessment (reading, spelling, phonological awareness), often complemented by a psychologist (cognitive testing) and an ENT specialist (hearing). | Multidisciplinary team: speech-language pathologist (SLP), ENT, paediatric neurologist, sometimes psychologist. Specialised reference centre for complex cases. |
| Course without intervention | Compensation possible but cognitively costly. Risks for school progress, fatigue, loss of confidence. Persists into adulthood in a more discreet form. | Persists into adulthood. Without therapy, oral language remains structurally limited; this also affects reading, writing and overall learning. |
| Care pathway | Speech-language therapy targeted at reading, school accommodations (extra time, oral reading of instructions). In France: PAP or PPS, the US equivalent is a 504 plan or IEP. | Intensive and early speech-language therapy, often several sessions per week. School accommodations frequently needed (in France: AESH classroom aide, ULIS class, PPS via the MDPH disability authority, US equivalent: IEP with related services). |
| Heredity | Strong genetic component: a child with a dyslexic parent has a 30 to 50% risk of being dyslexic too, depending on the study. | A genetic component is also present, more discreet. Undiagnosed language disorders are often found in the family history. |
| Co-occurrence with other disorders | Common with dysorthographia (spelling disorder), dyscalculia, ADHD. A child is rarely “only” dyslexic. | Very common with verbal dyspraxia, attention disorders, secondary dyslexia at school entry. DLD often “opens the door” to other difficulties. |
| Administrative recognition | Generally a PAP (school-internal accommodation plan); PPS and MDPH disability recognition for severe forms. FR-specific; US equivalent: 504 plan or IEP. | Most often PPS and MDPH recognition, given the severity and duration. FR-specific; US equivalent: IEP with related services. |
Sources: French national health authority (HAS) recommendations on specific language and learning disorders; Inserm collective expert review on dyslexia and SLD; FFDys (French DYS Federation); CATALISE international consensus.
FIRST DEFINITION
Dyslexia: a reading disorder, not an intelligence problem
Dyslexia is a specific, persistent neurodevelopmental disorder of reading acquisition. The dyslexic child has normal, sometimes above-average, intelligence, but the brain network that links a heard sound to a written sign does not wire up the way it does in other children.
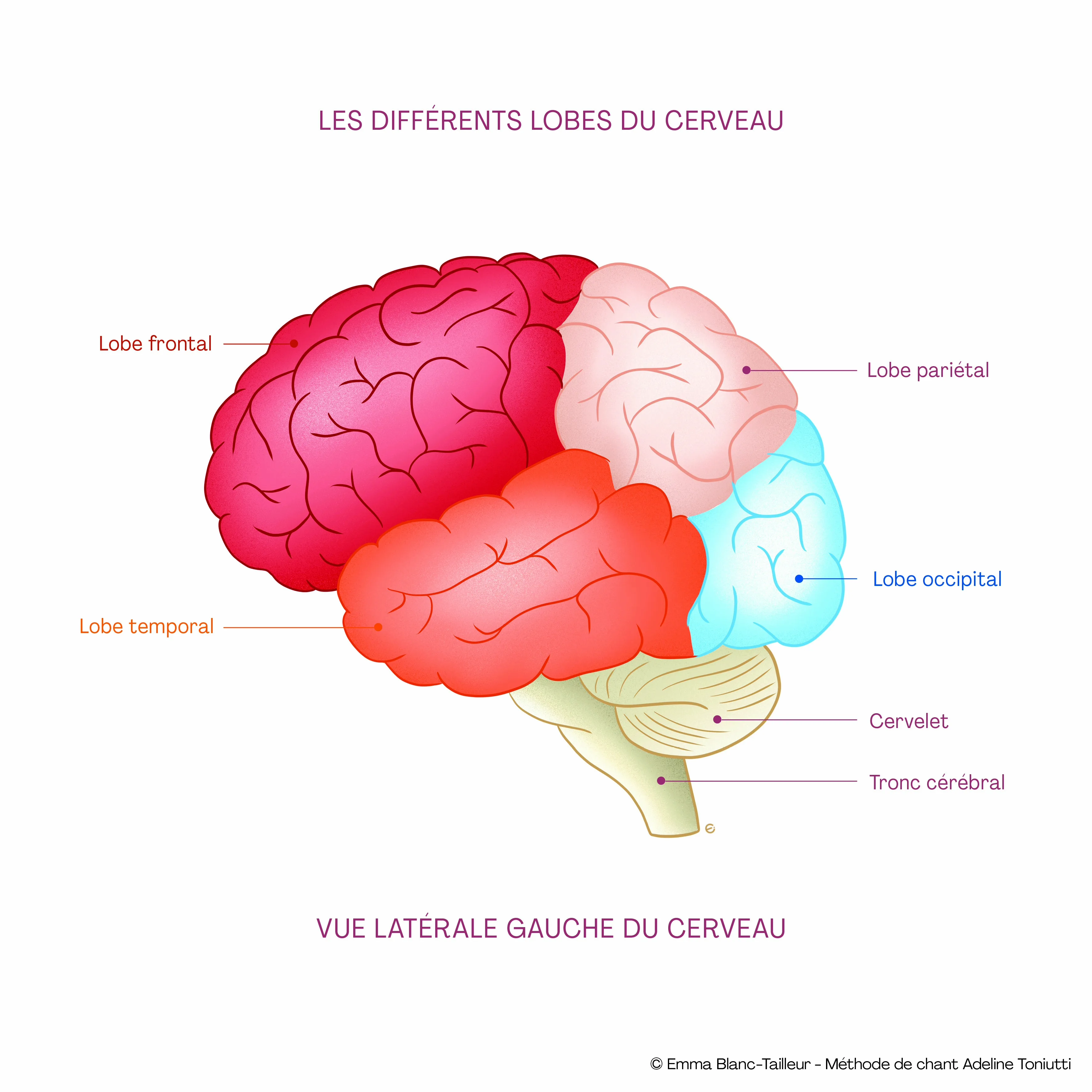
Concretely: your child inverts syllables (“basket” becomes “baksit”), confuses mirror letters (b/d, p/q), reads slowly, loses their line, gets tired after ten minutes of reading. Spelling stays unstable even after two years of school. It is not a lack of effort; it is a different brain wiring located in the left temporo-parietal circuits, where the brain associates sounds with letters.
Diagnosis is made after at least 18 months of formal reading instruction, usually around age 7-8. Before that, we do not speak of dyslexia: we speak of predictive signs (difficulty splitting words into syllables, recognising rhymes, memorising letter names).
© Emma Blanc Tailleur
SECOND DEFINITION
Dysphasia (DLD): a structural disorder of oral language
Dysphasia is a structural, persistent disorder of oral language, present from early childhood. The official term in the international literature today, following the 2017 CATALISE consortium consensus, is Developmental Language Disorder (DLD), but “dysphasia” remains the word used in most French clinics.
Here, the difficulty is not reading; it is building oral language itself. The child with DLD has a poor vocabulary for their age, builds sentences in a telegraphic style (“me no want eat”), distorts words (“pasghetti” for spaghetti), or sometimes does not understand a multi-step instruction even when articulated slowly. The expressive form is the most visible; the receptive form is rarer and more severe.
At the brain level, an atypical development of the left temporal and frontal areas is observed, Broca's area (production), Wernicke's area (comprehension) and their connecting tracts. This is neither a simple delay, nor an intelligence deficit, nor a parenting issue. Without intervention, dysphasia persists into adulthood.
HOW THE TWO ARE LINKED
Why a child with DLD often becomes dyslexic at school entry
A figure many parents do not know: about one child in two with dysphasia (DLD) develops dyslexia when learning to read. This is not chance. Reading rests on oral language. For a child to learn to read “cat”, they must first hear that the word “cat” is made up of two distinct sounds (/k/ and /æt/), that is what is called phonemic awareness. If oral language is itself fragile, reading is built on sand.
Hence a simple clinical rule: the earlier DLD is identified, the more early speech-language therapy can mitigate the dyslexia that risks appearing later. Conversely, some children labelled “dyslexic” at school entry actually have a DLD that went unnoticed in early childhood, because they were “quiet” or “reserved”, a structural disorder mistaken for a personality trait.
The “dys-” family is broad and often overlapping: dyslexia (reading), dysphasia / DLD (oral language), dysorthographia (spelling), dyscalculia (maths), dyspraxia (coordinated gestures, including verbal dyspraxia / Childhood Apraxia of Speech which affects motor planning of speech), dysgraphia (handwriting). A child rarely has just one. That is why a comprehensive assessment is worth more than a series of separate ones.
CARE PATHWAY
How to tell them apart in your own child
Three questions to ask yourself, and three professionals to consult, in order.
Before age 5: focus on oral language
If at age 3 your child does not make 3-word sentences, if at age 4 people outside the family cannot understand them, if at age 5 syntax is still telegraphic: first appointment with a speech-language pathologist (SLP). No later. No “wait and see, it will come”. Beforehand, a hearing test with an ENT specialist to rule out a mild bilateral hearing loss, common and underdiagnosed.
Around ages 6-8: focus on reading
Very slow, choppy reading, b/d confusion, spelling still very unstable after 18 months of instruction: SLP assessment with a specific “reading” battery. The assessment evaluates phonological awareness, reading speed, text comprehension, lexical and grammatical spelling. A school psychologist may add a cognitive assessment to frame the diagnosis.
If the picture is complex
Several “dys-” suspected at once, neurological history, severe DLD: referral to a specialised reference centre for language and learning disorders, or paediatric neurology consultation. The paediatric neurologist does not “treat” DLD but checks that no neurological disorder has been missed and coordinates the team.

THE CALYP ANGLE
Singing: a complement that strengthens what these two disorders weaken.
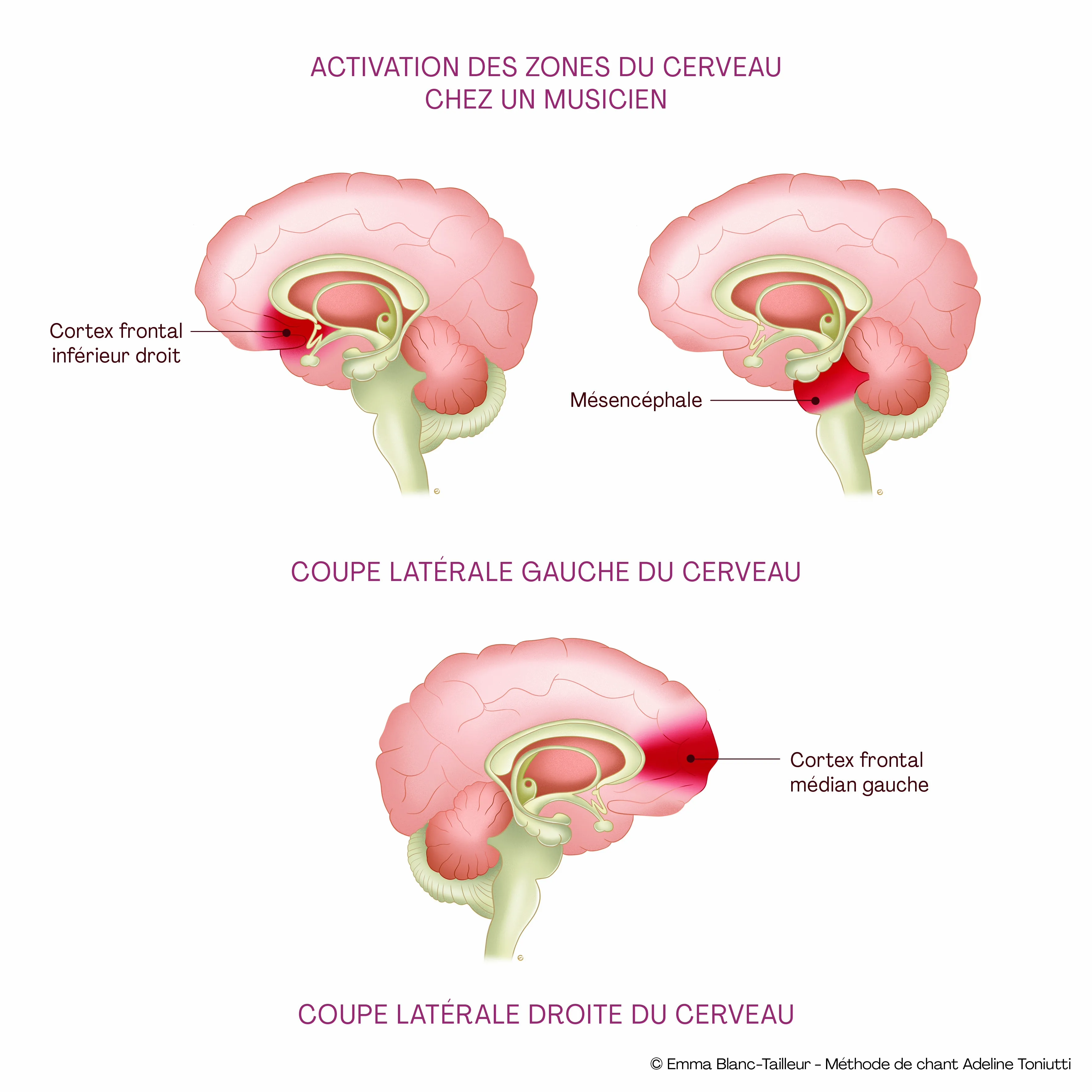
Singing is a remarkable trigger for progress, for brain activity as much as for body and emotion.
WHAT SINGING DOES, CONCRETELY
For dyslexia, for dysphasia (DLD)
For dyslexia: building phonemic awareness
Reading means linking a sound to a written sign. In a vocal warm-up like “ga-ga-ga”, the child hears the /g/ sound detached, clean, several times in a row. They feel in their mouth the movement of the back of the tongue propelling the sound upward. The articulatory gesture becomes conscious, and phonemic awareness is precisely one of the deficient functions in the dyslexic reader.
Vocal exercises on sibilants (F, S, SH), nasals (M, N) and propulsive consonants (G, K, R) train the child's ear to distinguish similar sounds that writing represents with similarly close letters.
For dysphasia (DLD): structuring oral language
The child with DLD often has a choppy delivery and a poor vocabulary. Singing imposes an external rhythmic frame, the song's pulse holds the sentence in place. Over an 8-bar nursery rhyme, the child learns a complete syntax without realising it, because melody and rhythm act as crutches for grammar.
The repetition of choruses builds an auditory memory of correct language. And the tongue-larynx pairing, put to work by articulation exercises, helps train the motor planning of speech, useful in children who also present with verbal dyspraxia.
The CALYP method was built in concertation with a multidisciplinary scientific committee, ENT surgeons, phoniatricians, speech-language pathologists, physiotherapists, psychiatrists. No session begins without clinical framing, and the work is always done in complement to ongoing medical and SLP follow-up.
FREQUENTLY ASKED QUESTIONS
Dyslexia or dysphasia: what parents ask us
Can my child have both dyslexia and dysphasia (DLD)? +
Yes, and it is common. About one child in two with DLD develops dyslexia when learning to read. In that case, care must target both levels: oral language first, because it serves as the foundation, then reading in parallel. A single speech-language pathologist can follow both axes if the assessment was properly cross-checked.
At what age can dyslexia be diagnosed? +
Not before around age 7-8. Diagnosis requires at least 18 months of formal reading instruction to distinguish a true persistent disorder from a slow start. Before that, we speak of predictive signs (difficulty with rhymes, syllables, letter names) and we can begin preventive intervention without using the word “dyslexia”.
At what age can dysphasia (DLD) be diagnosed? +
A firm diagnosis is generally made between ages 4 and 6, after several repeated assessments showing that the language delay does not resolve despite stimulation. But the first warning signs are visible much earlier: a 2-year-old who does not say about ten words, a 3-year-old who does not make 3-word sentences, that is already grounds for an SLP assessment. The rule: do not wait.
Can dysphasia (DLD) be cured? +
No, in the medical sense. Dysphasia is a structural disorder that persists into adulthood. But with early, intensive and well-led speech-language therapy, the child compensates considerably: they develop functional oral language, follow an adapted school path, become an independent adult. Many adults formerly identified with DLD lead very accomplished careers, sometimes without their current circle suspecting their childhood diagnosis.
Does dyslexia disappear in adulthood? +
No, but it is compensated. The dyslexic adult reads at a normal pace for their job, makes few visible mistakes, but often pays a hidden cost: cognitive fatigue, difficulty with foreign languages, spelling that remains a sensitive area. Recognising a child's dyslexia early spares the future adult from putting all their energy into camouflage.
What is the difference between dysphasia (DLD) and verbal dyspraxia? +
Dysphasia affects the conception of language: vocabulary, syntax, comprehension. Verbal dyspraxia (Childhood Apraxia of Speech) affects the motor production of sound: the child knows what they want to say but their tongue, lips and larynx do not coordinate the gesture correctly. The two can coexist in the same child, and it is precisely on the motor planning of speech that vocal work brings a useful complement.
Is my child dyslexic or simply slow to read? +
Three criteria to examine: duration (does the delay persist beyond 18 months of instruction?), gap (does the gap to the average exceed 18 months as measured on the assessment?), and specificity (are the other learning areas, maths, reasoning, within the norm?). If all three are checked, we speak of dyslexia. Otherwise, simple delay that catches up with adapted stimulation.
Can singing replace speech-language therapy? +
No, never. The speech-language pathologist is the health professional who makes the diagnosis, monitors progress, and has the widest range of exercises for language disorders. Singing intervenes as a complement: it provides a rhythmic and emotional frame that the SLP session cannot always offer, and it engages the four pillars at once (breathing, rhythm, articulation, auditory memory). At CALYP, we always work in liaison with the child's SLP.
How do I know whether to consult an SLP or a paediatric neurologist? +
The speech-language pathologist is the first point of contact in the vast majority of cases. The paediatric neurologist intervenes if the picture is complex: several specific learning disorders associated, neurological history (prematurity, seizures, trauma), suspicion of a broader syndrome. The family doctor or paediatrician makes the referral. There is no benefit in skipping steps by going straight to a paediatric neurologist for a difficulty that will be handled in speech-language therapy.
Are dyslexia or dysphasia hereditary? +
A hereditary component is documented for both, more pronounced for dyslexia: a child with a dyslexic parent has a 30 to 50% risk of being dyslexic too, depending on the study. For dysphasia, undiagnosed language disorders are often found in the family among parents or siblings. A family history is a serious reason to consult early, without waiting for difficulties to settle in.
SOURCES & REFERENCES
Scientific sources for this page
All factual claims (definitions, prevalence, neuroanatomy, heredity, care pathway, school provisions) come from peer-reviewed sources and verified institutional recommendations.
Official recommendations
- Haute Autorité de Santé (HAS), How to improve the care pathway of a child with specific language and learning disorders, Care pathway guide, December 2017 (FR). View on HAS
- Inserm, Collective expert review, Dyslexia, dysorthographia, dyscalculia: review of scientific data, Inserm Editions, Paris, 2007. iPubli Inserm summary
- American Psychiatric Association, DSM-5: Diagnostic and Statistical Manual of Mental Disorders, 5th edition, 2013. Specific learning disorder with reading impairment (315.00 / F81.0); Language disorder (315.39 / F80.2). APA description
Scientific consensus on terminology (CATALISE)
- Bishop DVM, Snowling MJ, Thompson PA, Greenhalgh T & CATALISE-2 consortium, Phase 2 of CATALISE: a multinational and multidisciplinary Delphi consensus study of problems with language development: Terminology, Journal of Child Psychology and Psychiatry, 2017; 58(10): 1068-1080. View on PubMed
- Bishop DVM, Snowling MJ, Thompson PA, Greenhalgh T & CATALISE consortium, CATALISE: A Multinational and Multidisciplinary Delphi Consensus Study. Identifying Language Impairments in Children, PLoS ONE, 2016; 11(7): e0158753. View on PubMed
- Bishop DVM & Snowling MJ, Developmental dyslexia and specific language impairment: same or different?, Psychological Bulletin, 2004; 130(6): 858-886. View on PubMed
Peer-reviewed: neurobiology of reading and language
- Shaywitz SE & Shaywitz BA, Dyslexia (specific reading disability), Biological Psychiatry, 2005; 57(11): 1301-1309. View on PubMed
- Shaywitz BA, Shaywitz SE et al., Functional disruption in the organization of the brain for reading in dyslexia, PNAS, 1998; 95(5): 2636-2641. View on PubMed
- Nasios G, Dardiotis E, Messinis L, From Broca and Wernicke to the Neuromodulation Era: Insights of Brain Language Networks for Neurorehabilitation, Behavioural Neurology, 2019. View on PubMed
Peer-reviewed: comorbidities, genetics & care
- Snowling MJ, Hayiou-Thomas ME, Nash HM, Hulme C, Dyslexia and Developmental Language Disorder: comorbid disorders with distinct effects on reading comprehension, Journal of Child Psychology and Psychiatry, 2020; 61(6): 672-680. View on PubMed
- Snowling MJ, Duff FJ, Nash HM, Hulme C, Developmental Outcomes for Children at High Risk of Dyslexia and Children With Developmental Language Disorder, Child Development, 2019; 90(5): e548-e564. View on PubMed
- Tomblin JB et al., Prevalence of specific language impairment in kindergarten children, Journal of Speech, Language, and Hearing Research, 1997; 40(6): 1245-1260. Seminal epidemiological study: prevalence 7.4%. View on PubMed
- Norbury CF et al., The impact of nonverbal ability on prevalence and clinical presentation of language disorder, Journal of Child Psychology and Psychiatry, 2016; 57(11): 1247-1257. DLD prevalence ~7.58%. View on PubMed
- Erbeli F, Rice M, Paracchini S, Insights into Dyslexia Genetics Research from the Last Two Decades, Brain Sciences, 2021; 12(1): 27. Heritability synthesis ~40-60%. View on PMC
- Doust C, Fontanillas P, Eising E et al., Discovery of 42 genome-wide significant loci associated with dyslexia, Nature Genetics, 2022; 54(11): 1621-1629. View on Nature Genetics
- Conti-Ramsden G, Durkin K, Simkin Z, Knox E, Specific language impairment and school outcomes, International Journal of Language & Communication Disorders, 2009; 44(1): 15-35. View on PubMed
- Adlof SM & Hogan TP, Understanding Dyslexia in the Context of Developmental Language Disorders, Language, Speech, and Hearing Services in Schools, 2018; 49(4): 762-773. View on PubMed
This page is for information only. It does not replace individual medical advice. For diagnosis or treatment, please consult a speech-language pathologist, a physician, or a specialised reference centre for language and learning disorders.
GET IN TOUCH
Book a first session
At CALYP, sessions are playful, designed to give children confidence in an artistic, positive and caring setting, and to spark new progress through what the musical gesture brings out. As a complement to speech-language therapy, never a replacement. First discovery session with Adeline or a coach trained in the CALYP method, in person in Paris or remotely.
Take a first lessonGOING FURTHER
Explore the topic further
PARENT PAGE
Language disorders
Overview: language delay, dyslexia, dysphasia, ADHD, dyspraxia. The CALYP method and the underlying neuroscience.
VOICE CLINIC
Voice Clinic
A medically-informed approach to the voice for adults and children, in liaison with ENT specialists, phoniatricians and speech-language pathologists.
FIRST SESSION
Book a session
Take a first lesson with Adeline or a coach trained in the CALYP method, in person in Paris or remotely.
METHOD
Adeline Toniutti
Vocal coach, founder of CALYP, author and creator of the Anatomy of Singing method.