Language delay in children: when should you consult?
LANGUAGE DISORDERS
Language does not develop at the same pace in all children. But there are precise milestones that help distinguish a normal variation from a signal that warrants a professional opinion.
WHAT YOU WILL FIND HERE
Your child is 22 months old and still doesn't say "dada". Their cousin, the same age, is already making sentences. You're typing "language delay" at 11 PM, telling yourself you might be overreacting. You're not overreacting, and you're not too late either. This page brings together precise developmental milestones (at 12 months, 18 months, 2 years, 3 years), the signals that justify a consultation, and the right order in which to consult. Without dramatising. Without minimising either.
CLINICAL MILESTONES
The language development timeline
The ages indicated are averages. A gap of a few months remains common. What matters is the sequence of stages, more than the exact date.
0–3 months
Cooing
The child produces sustained vowel sounds ("aaah", "oooh"). They make eye contact, smile in response, turn their head toward familiar voices. A newborn's larynx, as Adeline Toniutti's vocal method describes it, stays extraordinarily mobile: it can cry for hours without tiring.
4–7 months
Babbling
Consonants appear: "ba", "ma", "da", "ga". The child plays with their mouth, tongue, and lips. They imitate the intonations they hear. Babbling responds to the maternal voice, in a body-to-body mechanism described by Dr. Jean Charmoille (psychiatrist, child psychiatrist).
8–12 months
Proto-words
The child strings syllables together: "papapapa", "mamamama". These sounds are not yet words with stable meaning. They point with their finger, shake their head for "no", recognise their name. Around 12 months, some children say their first intentional words.
12–18 months
First referential words
"Mama" refers to mama, "woof" refers to the dog. At 18 months, the child understands far more words than they produce (between 50 and 100 words understood versus 10 to 50 spoken). They follow simple instructions: "bring me your shoe".
18–24 months
The lexical explosion
Vocabulary jumps from 50 to 200 words in just a few months. First two-word combinations appear: "daddy gone", "apple more". By 24 months, the child produces an average of 200 to 300 words and starts using "me" or their first name.
2–3 years
Sentences
Three- to four-word sentences: "me want apple", "daddy gone work". Vocabulary climbs to 500–1,000 words. The child asks their first questions ("what's this?"). Speech remains imperfectly articulated: that's normal.
3–4 years
Basic grammar
The child uses "I" correctly, conjugates verbs in the present tense, recounts what they did at school. They ask "why?" relentlessly. Their speech is understood by an unfamiliar adult about 75% of the time.
4–5 years
Structured narrative
The child tells a story with a beginning, a middle, and an end. They master common conjugations and almost all sounds (the "r" and "ch" may still lag). They play with rhymes, nursery rhymes, and verbal humour.
5–6 years
Entry into reading
Phonology is acquired (all sounds in the language produced correctly), syntax is complex, vocabulary is rich. The child enters early reading. This is the age when dyslexia reveals itself at school. DLD (Developmental Language Disorder, formerly dysphasia) is generally identified earlier, around 3–4 years.
A POINT OF VOCABULARY
"Delay" and "disorder" do not mean the same thing
A language delay is a gap in time. The child is on the right path, simply later. With appropriate stimulation and a little patience, they catch up with their peers. This is the most frequent situation, and the one that worries parents the most unnecessarily.
A language disorder is an atypical development that persists despite stimulation. It may be DLD (Developmental Language Disorder), a specific articulation disorder, a disorder linked to a hearing impairment or to autism spectrum disorder. An assessment by a speech-language pathologist (SLP), sometimes complemented by a multidisciplinary opinion, allows a diagnosis to be made.
For the detailed distinction and the list of specific disorders, see the page Language disorders in children and adolescents.
WARNING SIGNS
When should you consult?
None of these signals automatically means "disorder". All warrant a professional opinion. A reassuring assessment puts your mind at ease; an early-detection assessment can save years.
AT 12 MONTHS
The child does not babble with consonants. They imitate neither intonations nor simple gestures (waving goodbye, clapping). They do not respond to their name.
AT 18 MONTHS
No words produced with clear intent. They do not point to request or to show. They do not understand simple instructions without an accompanying gesture.
AT 24 MONTHS
Fewer than 50 words produced, no two-word combinations, vocabulary that has not increased for several months.
AT 3 YEARS
Speech is unintelligible even to close family. They do not form sentences. They do not ask questions.
AT 4 YEARS
Persistent ungrammatical sentences ("me go school tomorrow daddy"), major sound distortions, poor vocabulary. Difficulty recounting what happened during the day.
AT ANY AGE
A regression: your child loses words they had acquired, abandons eye contact, withdraws. This sign warrants a rapid consultation, without waiting for the next pediatric visit.
THE PATHWAY
Who to consult, and in what order?
General practitioner or pediatrician
First point of contact. They ask questions, observe the child, prescribe the necessary assessments. They will refer you to the appropriate specialists. The prescription for a speech-language assessment goes through them.
ENT specialist with audiogram
Almost always the first-line step. The aim is to rule out mild hearing loss, chronic glue ear (otitis media with effusion), or an anatomical defect. A child who does not hear well cannot reproduce what they cannot hear. Many apparent delays are explained by imperfect hearing and resolve with grommets or rehabilitation.
Speech-language pathologist (SLP)
The speech-language assessment evaluates production, comprehension, non-verbal communication, and symbolic play. It lasts between one and three hours, sometimes spread over several sessions. In France, it is reimbursed at 60% by national health insurance with a medical prescription (private insurance generally covers the rest). At the end, the SLP makes a diagnosis and proposes regular follow-up if needed (often one to two sessions per week).
If needed: pediatric neurologist, psychomotor therapist, psychologist
An isolated language disorder is common. When it is accompanied by motor, attentional, or relational difficulties, the SLP refers to a multidisciplinary assessment. The pediatric neurologist evaluates the neurological dimension; the psychomotor therapist the motor and sensory dimension; the psychologist the cognitive and emotional dimension.
UNDERSTANDING THE ORIGINS
Where does a language delay come from?
Causes often overlap. Identifying the main one changes the prognosis.
- Auditory. Recurrent middle-ear infections, mild or unilateral hearing loss. This is the simplest cause to correct and the most frequent.
- Neurological or neurodevelopmental. DLD (Developmental Language Disorder), autism spectrum disorder, sequelae of prematurity, perinatal lesions.
- Genetic. Family history of language delay, dyslexia, or DLD. The hereditary weight is real without being deterministic.
- Global cognitive. When the language delay is part of a broader developmental delay.
- Environmental. Lack of verbal stimulation, screen overexposure before age 3, emotional instability, social isolation. Language is built through exchange: without an interlocutor, it fades.
One last point that many parents forget: well-supported bilingualism does not create language delay. Temporary confusion between two languages is normal and resolves itself. What creates delay is poor and unstable exposure, in one language or in two.
THE SPECIALIST'S INSIGHT
Language begins with the maternal voice
The work Adeline Toniutti has carried out with the doctors and specialists who support her vocal method draws in particular on the insight of Dr. Jean Charmoille, psychiatrist, child psychiatrist and psychoanalyst, honorary vice-president of CALYP, into the mechanics of language at its very first moments.
Babbling, he explains, is the child's response to the mother's first words, in a context of body-to-body contact. Through that babbling, the child perceives less the meaning of words than the breaks that give the maternal language its rhythm. It is through those breaks that the child responds and gradually enters their mother's language.
Dr. Charmoille also recalls a famous historical anecdote reported by the chronicler Salimbene de Adam in the 13th century: Emperor Frederick II, convinced that an original language existed, is said to have had infants raised by nurses forbidden to speak to them. None reportedly survived to develop language. The story, whose authenticity remains debated by historians, symbolically illustrates that without a voice addressing them, the child does not enter language. And not just any voice: a voice that takes an interest in them, that modulates, that almost sings.

© Emma Blanc Tailleur
AT HOME
Five simple gestures to stimulate language
These gestures do not replace an assessment if you have doubts. But they nourish the ground on which language grows, and they are free.
1.
Talk a lot, and slowly
Describe what you are doing. "I'm cutting the apple. See, the apple is red. Now I'm putting it in your bowl." This seemingly mundane stream is what the child's brain needs to map their language.
2.
Read one book a day
A picture book at 12 months, a short story at 2 years, a narrative at 4 years. Point to the pictures, name them, repeat. Children who are read to regularly enter school with a noticeably richer vocabulary than the average, measured gaps between first-grade pupils vary by a factor of one to five depending on language exposure (CSEN, the French Scientific Council for Education; Réseau Canopé, the French national education resource network).
3.
Sing, and have them sing
Nursery rhymes, lullabies, car singalongs. Singing trains rhythm, articulation, auditory memory and breathing all at once. Melody creates a rail on which words attach. Children remember the words of a song long before they remember an equivalent spoken text.
4.
No screens before age 3
The WHO, the French High Council for Public Health (HCSP), and pediatric societies repeat it: passive screen time brings nothing to language before age 3, and many slow it down. The problem is not the content, it's the time taken away from human interaction.
5.
Put words on emotions
"You're angry because your brother took your truck." "You're sad because grandma left." Naming an emotion gives the child the tool to move through it rather than endure it. And it's also very high-density vocabulary.
IF YOU REMEMBER ONLY ONE
A child who does not hear a voice that takes an interest in them does not learn to speak. The rest is secondary.
© Emma Blanc Tailleur
THE CALYP APPROACH
Singing as a complement to speech therapy
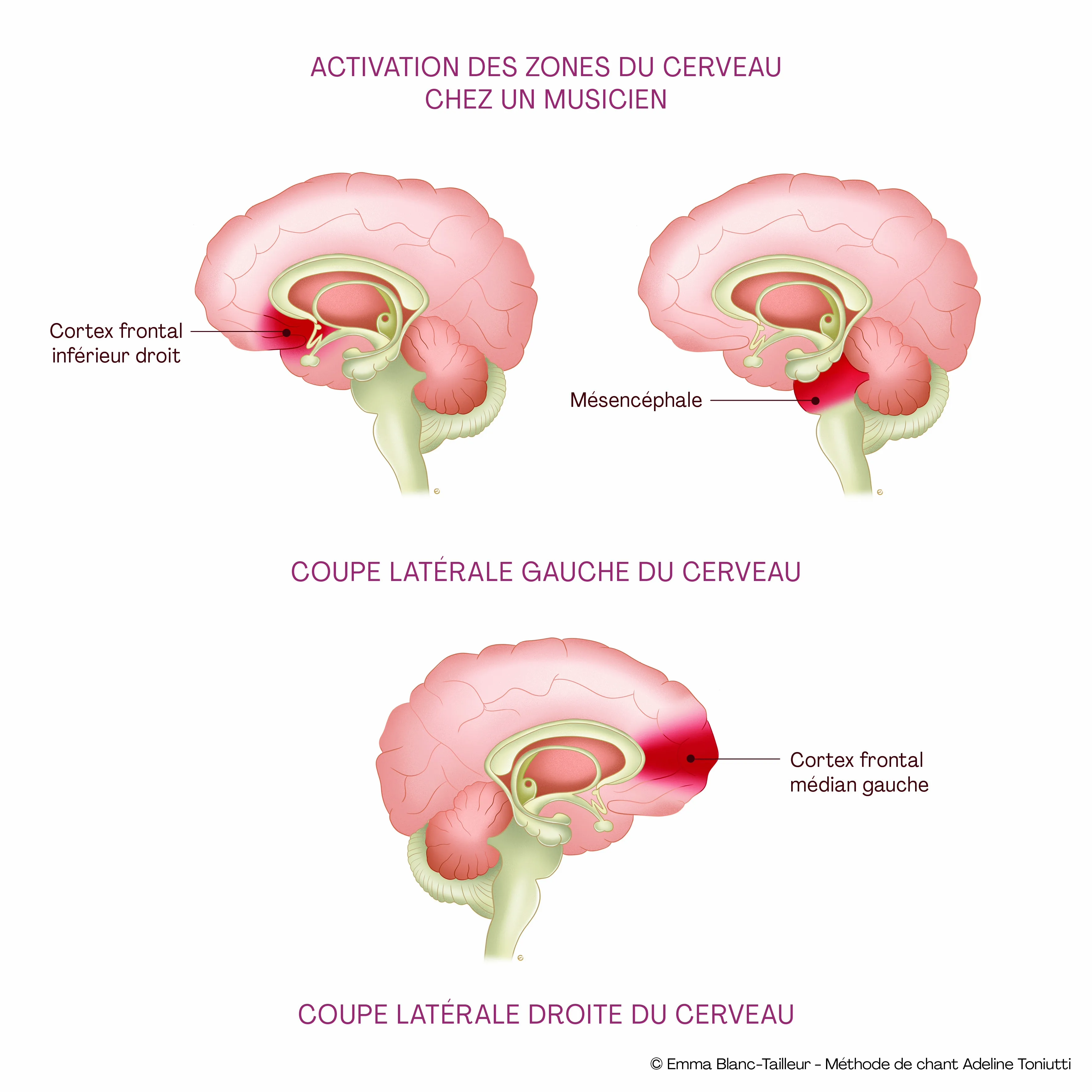
A clinical observation supported notably by post-stroke aphasia in adults (Melodic Intonation Therapy): a patient who cannot say a word can sometimes sing it. This dissociation is due to the fact that speech and singing do not entirely use the same brain circuits. Singing mobilises both hemispheres more equally; speech relies more heavily on the left hemisphere. In children, singing can, in the same spirit, offer a motivating point of entry when access to speech is difficult.
At CALYP, singing is never presented as a treatment that replaces speech therapy. It comes as a complement, and it opens a door that classical speech therapy sometimes struggles to push: the door of pleasure. A child who drags their feet into a speech therapy session can run into a singing session. This difference in motivation can fuel the overall dynamic of care.
The support relies on familiar nursery rhymes, songs the child chooses, vocal games on vowels, exercises imitating intonations. The 5 pivot points method developed by Adeline Toniutti in Anatomie du Chant (validated with 26 doctors and specialists) provides the technical framework: posture, laryngeal movement, exhalation, resonance, articulation. Adapted to age, these points become bodily games.
GET IN TOUCH
Book a first lesson
At CALYP, lessons are playful and rebuild children's confidence in an artistic, positive and caring setting, sparking new progress through the qualities of musical gesture. As a complement to medical and speech-therapy follow-up, never in their place. First discovery session with Adeline or a coach trained in the CALYP method, in person in Paris or remotely.
Book a first lessonFREQUENTLY ASKED QUESTIONS
Your questions, briefly
My child is 22 months old and only says "mama" and "dada". Should I consult? +
Yes, talk about it with the pediatrician at the next visit. By 24 months, the average is around 50 words and first two-word combinations. Below that, the pediatrician will refer for an audiogram and, if needed, a speech-language assessment. Many late talkers catch up; identifying them sooner means saving time when a disorder is involved.
At what age should a child say their first word? +
First words with clear intent ("dada" referring to dad, not just anyone) appear on average around 12 months. A range of 9 to 15 months remains common. The complete absence of words at 18 months warrants medical advice.
What is the lexical explosion? +
A sudden acceleration of vocabulary between 18 and 24 months. The child goes from 50 words to 200, then 300 in just a few weeks. They start combining two words. This explosion does not happen in all children at the same time; it can occur later without being pathological.
Does bilingualism delay my child's language? +
No, provided exposure is rich and stable in both languages. Occasional mixing of words between two languages is normal and resolves itself. A well-supported bilingual child reaches the same language milestones as a monolingual one, sometimes with a slight gap that catches up before school.
How long does a speech-language assessment take? +
On average one hour, sometimes two sessions. In France it is reimbursed by national health insurance with a medical prescription. At the end, the SLP writes a detailed report and proposes follow-up if needed. The waiting time for an appointment can be long; ask for the prescription as soon as doubt appears.
My child understands everything but does not speak. Is this concerning? +
It is actually rather reassuring: the gap between comprehension and production is normal in young children (children always understand more words than they say). But if the gap widens beyond normal ages and production remains very limited at 24 or 30 months, an assessment is warranted.
Can screens really cause language delay? +
They do not cause a disorder, but they can generate or worsen a delay. The mechanism is not the screen content: it's the time taken away from human interaction. A child who spends two hours a day in front of a screen spends two hours less hearing someone speak to them. Before age 3, passive screen time has no proven benefit on language.
Can ear infections slow down language development? +
Yes, and it's one of the most underestimated causes of language delay. Chronic glue ear (otitis media with effusion) between 12 and 36 months causes fluctuating hearing loss: the child hears sounds as if they had cotton in their ears. They cannot reproduce what they do not hear correctly. An ENT consultation with audiogram is systematic in case of delay.
Can singing really help a child who is not speaking? +
It helps as a complement to speech therapy, never as a replacement. A child who struggles to articulate a word can sometimes sing it, because melody activates brain circuits that only partially overlap with those of speech. At CALYP, singing serves as a playful entry point to work on rhythm, articulation, breathing. Progress in singing can then nourish speech.
My older child spoke late, my younger one too: is it genetic? +
A predisposition exists: children whose parent or sibling has had a language delay are more likely to present one too. This does not exempt you from consulting. On the contrary, family history justifies heightened vigilance, especially if the older child eventually needed speech therapy.
My child is regressing: they had words, they're losing them. What should I do? +
Language regression warrants a quick consultation, without waiting for the next pediatric visit. It can accompany autism spectrum disorder, neurological involvement, a major emotional event. The pediatrician will refer to the appropriate specialists. The earlier the care, the better the prognosis.
Should I force the child to repeat when they pronounce poorly? +
No. Forcing repetition creates inhibition, and a child who feels constantly corrected ends up speaking less. The recommended technique is recasting: they say "tato", you reply "yes, that's your potato, shall we eat it?". You offer the correct model without correcting them. They will integrate it on their own.
SOURCES & REFERENCES
Scientific sources for this page
All claims come from peer-reviewed sources and verified institutional recommendations.
Developmental milestones & official recommendations
- Haute Autorité de Santé (HAS, French High Authority for Health). Neurodevelopmental disorders, identification and referral of at-risk children. Best practice recommendations, February 2020. has-sante.fr
- Haut Conseil de la Santé Publique (HCSP, French High Council for Public Health). Child health record, update recommendations. Opinions and reports, 2017–2018. hcsp.fr
- French Society of Ambulatory Pediatrics (AFPA). ERTL4 toolkit, screening for language disorders at age 4. afpa.org
- French Society of Ambulatory Pediatrics (AFPA). D.P.L.3 toolkit, early screening for language disorders at age 3. afpa.org
- Inserm (French National Institute of Health and Medical Research). Dyslexia, dysorthography, dyscalculia: review of scientific data. Collective expertise, Les éditions Inserm, Paris, 2007. ipubli.inserm.fr
- Inserm. Specific learning disorders. Information dossier. inserm.fr
- French Federation of Speech-Language Pathologists (FNO). FNO Prevention, 0–3 years booklet, oral language and warning signs. fno-prevention-orthophonie.fr
Peer-reviewed articles, language acquisition
- Fenson L, Dale PS, Reznick JS, Bates E, Thal DJ, Pethick SJ. Variability in early communicative development. Monographs of the Society for Research in Child Development, 1994; 59(5): 1–173. PubMed 7845413
- Werker JF, Tees RC. Cross-language speech perception: evidence for perceptual reorganization during the first year of life. Infant Behavior and Development, 1984; 7(1): 49–63. ScienceDirect
- Kuhl PK, Tsao FM, Liu HM. Foreign-language experience in infancy: effects of short-term exposure and social interaction on phonetic learning. PNAS, 2003; 100(15): 9096–9101. PNAS
- Romeo RR, Leonard JA, Robinson ST et al. Beyond the 30-Million-Word Gap: children's conversational exposure is associated with language-related brain function. Psychological Science, 2018; 29(5): 700–710. PubMed 29442613
Peer-reviewed articles, Developmental Language Disorder (DLD) & bilingualism
- Bishop DVM, Snowling MJ, Thompson PA, Greenhalgh T, CATALISE consortium. CATALISE: A Multinational and Multidisciplinary Delphi Consensus Study. Identifying Language Impairments in Children. PLoS ONE, 2016; 11(7): e0158753. PLOS ONE
- Bishop DVM, Snowling MJ, Thompson PA, Greenhalgh T, CATALISE-2 consortium. Phase 2 of CATALISE: a multinational and multidisciplinary Delphi consensus study of problems with language development: Terminology. Journal of Child Psychology and Psychiatry, 2017; 58(10): 1068–1080. PMC5638113
- Hoff E. Bilingual Development in Children of Immigrant Families. Child Development Perspectives, 2018; 12(2): 80–86. PubMed 29805472
- Hoff E, Core C. Input and Language Development in Bilingually Developing Children. Seminars in Speech and Language, 2013; 34(4): 215–226. PMC4457512
Peer-reviewed articles, otitis media, hearing & language
- Roberts JE, Rosenfeld RM, Zeisel SA. Otitis media and speech and language: a meta-analysis of prospective studies. Pediatrics, 2004; 113(3): e238–e248. PubMed 14993583
- Roberts JE, Burchinal MR, Zeisel SA. Otitis Media in Early Childhood in Relation to Children's School-Age Language and Academic Skills. Journal of Speech, Language, and Hearing Research, 2002. ASHA Journals
- Rovers MM, Straatman H, Ingels K et al. The effect of ventilation tubes on language development in infants with otitis media with effusion: a randomized trial. Pediatrics, 2000; 106(3): E42. PubMed 10969126
Peer-reviewed articles, singing, music and language (MIT)
- Norton A, Zipse L, Marchina S, Schlaug G. Melodic Intonation Therapy: shared insights on how it is done and why it might help. Annals of the New York Academy of Sciences, 2009; 1169: 431–436. PMC2780359
- Schlaug G, Marchina S, Norton A. Evidence for plasticity in white-matter tracts of patients with chronic Broca's aphasia undergoing intense intonation-based speech therapy. Annals of the New York Academy of Sciences, 2009; 1169: 385–394. PubMed 19673813
- Liu Q, Wang X, Liu D et al. Melodic Intonation Therapy on Non-fluent Aphasia After Stroke: a systematic review and analysis on clinical trials. Frontiers in Neuroscience, 2022; 15: 753356. PMC8829877
Parental recommendations, vocabulary & screens
- French Scientific Council for Education (CSEN), Réseau Canopé. How to facilitate vocabulary acquisition in pre-school? Research synthesis and recommendations, 2023. reseau-canope.fr
- Haut Conseil de la Santé Publique (HCSP). Effects of children's and young people's exposure to screens. Opinion of 12 December 2019. hcsp.fr
- Madigan S, McArthur BA, Anhorn C, Eirich R, Christakis DA. Associations Between Screen Use and Child Language Skills: A Systematic Review and Meta-analysis. JAMA Pediatrics, 2020; 174(7): 665–675. PubMed 32202633
- Madigan S, Browne D, Racine N, Mori C, Tough S. Association Between Screen Time and Children's Performance on a Developmental Screening Test. JAMA Pediatrics, 2019; 173(3): 244–250. PMC6439882
This page is for informational purposes. It does not replace individual medical advice.
GOING FURTHER
Explore the topic in depth
PARENT PAGE
Language disorders
Overview: dyslexia, DLD, ADHD, dyspraxia. The CALYP method, neuroscience, medical team.
VOICE CLINIC
Voice Clinic
CALYP's medical and pedagogical hub: neuroscience, voice specialists, multidisciplinary support.
GET IN TOUCH
Book a first session
First discovery session with Adeline or a coach trained in the CALYP method, in person in Paris or remotely.
FOUNDER
Adeline Toniutti
Vocal coach, founder of CALYP, author of Anatomie du Chant and La Bonne Voix.